Research & Reviews: Journal of Medical and Health Sciences
ISSN: 2319-9865
ISSN: 2319-9865
Sarbhjit Kaur1*, Vijay Kumar Bodal2, Manjit Singh Bal2, Ranjeev Bhagat2, Manjit Kaur Mohi1, and Jasmeen Kaur2
Department of Gynecology & Obstetrics, Government Medical College, Patiala, Punjab, India.
Department of Pathology, Government Medical College, Patiala, Punjab, India.
Received: 16 June 2013 Accepted: 07 July 2013
Visit for more related articles at Research & Reviews: Journal of Medical and Health Sciences
Xanthogranulomatous oophoritis is an unusual chronic inflammation and clinically it form a mass-like lesion in the pelvic cavity and invades the surrounding tissue which mimic the tumour. Histologically, it is characterized by the presence of lipid filled macrophages with admixed lymphocytes, plasma cells and neutrophils. Granulomatous change ocurrs in other organs like gall bladder, kidney etc and etiology is unknown
xanthogranulomatpus inflammation, oophoritis, salpingitis, endometritis
Xanthogranulomatous inflammation of the female genital tract is uncommon lesion, in the pelvic cavity that invades the surrounding tissues, which may mimic the tumour clinically and by imaging [1]. it is destructive to normal tissue of affected organs [2].
Xanthogranulomatous inflammation has been reported Only a few cases involving the ovary have been reported to date in India . We describe a rare case of Xanthogranulomatous oophoritis.
A 65 yr old multiparous, postmenopausal female presented to Gynaecology OPD, of our institution with complaints of bloating, retching and pain in the lower abdomen for one year. She has off and on fever for few days. On clinical examination, patient had a firm, non tender, oval mass in right iliac, lumbar and umbilical area. Laboratory tests showed elevated ESR and white blood cell count. Ultrasound showed right adnexal mass. CT guided FNAC revealed purulent material, polymorphonuclear cells and foamy macrophages along with lymphocytes in background of necrotic debris.
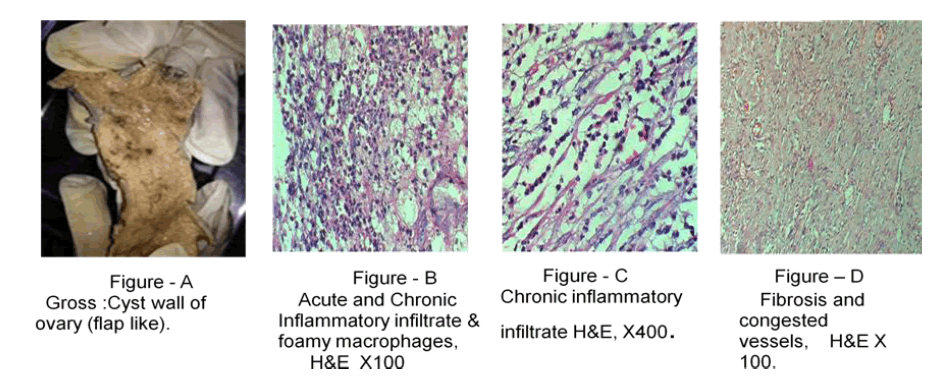
A flap like structure measuring 7.5x6.5x2 cm in size (figure A). Outer surface was yellowish with small nodule.
Examined multiple pieces show ovarian tissue infiltrated by acute as well as chronic inflammatory infiltrate consisting of many foamy macrophages with abundant cytoplasm and hypochromatic central nuclei, polymorphonuclear cells, some lymphoid cells and fibrosis (figure B&C). These foamy macrophages are scattered in various parts of lesion. The fibrosis is marked at places with hyalinisation. Many congested and thick walled blood vessels and hemorrhages are present (figure D).
Xanthogranulomatous oophoritis is often misdiagnosed by pathologists if they do not keep this entity in mind this may be due to the rarity of the condition. If the lesion is mainly focal scattered lymphocytes, it may be misdiagnosed as secondary lymphoma or leukemia. If the lymphocytes are scattering diffusely and foam cell are seldom, a diagnosis of malignant small cell tumour with stromal luteinzation may be rendered. If small amount of obivious fibrosis fibrosis and foam cells , a diagnosis of sclerosing stromal tumour may be made [3].
Correct diagnosis is made chiefly by histology, a suggestive preoperative diagnosis of xanthogranulomatous oophoritis could be lead to less radical surgery. The treatment of choice for Xanthogranulomatous oophoritis is oophrectomy. Patient with Xanthogranulomatous oophoritis should be monitor closely as it is associated with pelvic inflammatory diseases, endometriosis and intrauterine death [4,5,7].
The average age of patients of Xanthogranulomatous Oophoritis is 31 years. Although the pathogenesis of ovarian lesions is not fully understood, but proposed causes are infection, ineffective antibiotic therapy, abnormality in lipid metabolism, endometriosis or ineffective clearance of bacteria by phagocytes [8], rarely does a chronic ovarian abscess result in a solid tumor like mass, which is called either an ovarian Xanthogranuloma or Xanthogranulomatous oophoritis. This lesion occurs in patients with recurrent pelvic inflammatory disease. The involved ovary in each of the previously reported cases was replaced by a solid, yellow, lobulated mass that was well circumscribed and consisted of Xanthogranulomatous inflammation [6].
Hence, a diagnosis of Acute or Chronic Oophritis with Abundant Xanthogranulomatous Change was made. The case is being presented for its rarity.